Astra Tech
BioManagement Complex Astra Tech
BioManagement Complex
|
 Connective Contour Connective Contour
Connective Contour" is the unique and scientifically documented contour that increases soft tissue contact zone and volume, created when the abutment is connected to the implant. Connective Contour is also an original key feature of the Astra Tech Implant System™.
The summaries in this section highlight the understanding of soft tissue healing around and esthetics maintained by the Astra Tech Implant System.
 Tissue reactions to abutment shift: An experimental study in dogs Tissue reactions to abutment shift: An experimental study in dogs
Purpose: The aim of this experimental study was to evaluate tissue response following removal of healing abutments and placement of definitive abutments.
Material and Methods: The mandibular premolars of 6 beagle dogs were extracted 3 months prior to re-entry for insertion of three 8 x 3.5 mm Astra Tech implants bilaterally. Baseline radiographs were taken immediately after implant placement using a customized device to permit standardization. Cover screws were placed and flaps repositioned for submerged healing. After a further three months an exposure procedure was carried out via incision and flap elevation for removal of cover screws and location of healing abutments in two of the implants (Gl and G2) and a definitive uniAbutment in the third implant (Control). After a further two weeks the two healing abutments were replaced with a uniAbutment (Gl) and a Profile BiAbutment (G2). The latter had been prepared in a dental laboratory and then cleaned in an ultrasonic bath and autoclaved. Radiographs were taken again.
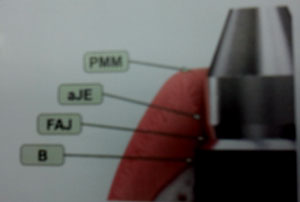
All abutments were subject to a rigorous cleaning regime and then were assessed clinically and radio-graphically after 3 and 6 months, at which point the animals were sacrificed. Their mandibles were removed en bloc to harvest the individual implants for preparation using the fracture technique to create a buccal and lingual tissue portion from around each implant, which were then further subdivided mesio-distally. Each quarter portion was fully decalcified, sectioned to 3 im and stained in periodic acid-Schiff and toluidine blue. Five sections from each of the four portions were used for histologic and histo-morphometric analysis to measure the position of the marginal mucosa (PMM), the apical termination of the junctional epithelium (aJE), the marginal bone-to-implant contact (BIC), the level of the fixture/abutment junction (FAJ) and the distances between these various landmarks. In addition the location and size of any inflammatory lesion was measured. Finally the content of collagen, vessels, fibroblasts, and residual tissue was calculated in a defined peri-implant zone.
Results: All implants osseointegrated, and the clinical examinations revealed a high degree of plaque control at all surfaces. Baseline marginal bone levels were similar for all three groups. Initial bone loss measured 0.7 mm to 0.9 mm after the first 6 months of plaque control. These changes were not significant between the control group and the two test groups, Gl and G2.
For histometric measurement the distances between various levels was comparable with PMM-B ranging from 3.11 mm to 3.25 mm, PMMaJE ranging from 1.72 mm to 1.76 mm, aJE-BIC ranging from 1.35 mm to 1.48 mm and FAJ-BIC ranging from 0.72 mm to 1.00 mm. The differences were again not significant. However the size of the inflammatory lesion was significantly bigger by area in the G2 group (0.64 mm2) compared to controls (0.07 mm2), (p < 0.05) and the Gl group (0.15 mm2),(p < 0.05). This infiltrate was well defined and consistently seen in the connective tissue compartment at the level of the FAJ and for G2 implants it extended lateral to the barrier epithelium. There was no significant difference between the proportion of vessels, collagen, fibroblasts and residual tissue between the groups.
Discussion: In the current study it can be concluded that abutment shifting from healing abutment to a permanent abutment did not compromise the mucosal attachment since the dimensions and character of the mucosal compartment were comparable and re-attachment was established. in addition, there was no notable change in marginal bone levels, which remained stable once equilibrium was established after exposure. These results are in general agreement with other studies.
The presence of an inflammatory infiltrate in the connective tissue compartment was routine and supports previous findings, however there was a significant increase in the area of the infiltrate for the G2 group which had their healing abutments changed for two-piece hollow prepable abutments. The increased infiltrate may have resulted from handling in the lab-oratory or due to the increased risk of microleakage that is thought to exist at hollow abutments.
|
|
|